| Identification | More | [Name]
L-Thyroxine | [CAS]
51-48-9 | [Synonyms]
3,3',5,5'-TETRAIODO-L-THYRONIN
3,3',5,5'-TETRAIODO-L-THYRONINE
3,3',5,5'-TETRAIODO-L-THYRONINE SODIUM SALT
3,5,3',5'-TETRAIODO-L-THYRONINE
l-2-amino-3-[4-(4-hydroxy-3,5-diiodo-phenoxy)-3,5-diiodo-phenyl]-propanoic acid
LEVOTHYROXINE
LEVOTHYROXINE SODIUM
L-THYROXIN
L-THYROXINE
L-THYROXINE NA
L-THYROXINE SODIUM
L-THYROXINE SODIUM SALT
O-(4-HYDROXY-3,5-DIIODOPHENYL)-3,5-DIIODO-L-TYROSINE
(S)-2-AMINO-3-[4-(4-HYDROXY-3,5-DIIODOPHENOXY)-3,5-DIIODOPHENYL]PROPIONIC ACID
T4
TETRAIODOTHYRONINE, NA
THYROXINE
3,5,3’,5’-tetraiodothyronine
beta-[(3,5-diiodo-4-hydroxyphenoxy)-3,5-diiodophenyl]alanine
l-3,5,3’,5’-tetraiodothyronine | [EINECS(EC#)]
200-101-1 | [Molecular Formula]
C15H11I4NO4 | [MDL Number]
MFCD00002596 | [Molecular Weight]
776.87 | [MOL File]
51-48-9.mol |
| Chemical Properties | Back Directory | [Appearance]
Crystalline Solid | [Melting point ]
235 °C | [alpha ]
-5 º (1N NaOH:EtOH 1:2) | [density ]
2.4440 (estimate) | [Fp ]
9℃ | [storage temp. ]
2-8°C
| [solubility ]
Dissolves in 4M ammonium hydroxide in Methanol at 50mg/ml | [Boiling point ]
576.3±50.0 °C(Predicted) | [form ]
Powder | [pka]
2.2(at 25℃) | [color ]
White to Pale Brown | [optical activity]
-4.5 to -5.7 [1 mol dm-3 NaOH-ethanol (1:2)] +15 [1 mol dm-3 HCl-95% ethanol (1:2)] | [Water Solubility ]
insoluble | [Sensitive ]
Light Sensitive | [Usage]
One of the thyroid hormones involved in the maintenance of metabolic homeostasis. Synthesized and stored as amino acid residues of thyroglobulin, the major protein component of the thyroid follicular colloid. Synthesis and secretion are regulated by | [Merck ]
9491 | [BRN ]
2228515 | [InChIKey]
XUIIKFGFIJCVMT-LBPRGKRZSA-N | [CAS DataBase Reference]
51-48-9(CAS DataBase Reference) | [EPA Substance Registry System]
51-48-9(EPA Substance) |
| Safety Data | Back Directory | [Hazard Codes ]
Xn | [Risk Statements ]
R40:Limited evidence of a carcinogenic effect. | [Safety Statements ]
S22:Do not breathe dust .
S24/25:Avoid contact with skin and eyes .
S36:Wear suitable protective clothing . | [RIDADR ]
UN1230 - class 3 - PG 2 - Methanol, solution | [WGK Germany ]
3
| [RTECS ]
YP2833500
| [F ]
8-10 | [TSCA ]
Yes | [HazardClass ]
IRRITANT | [HS Code ]
29379000 | [Hazardous Substances Data]
51-48-9(Hazardous Substances Data) | [Toxicity]
TDLo oral in child: 328ug/kg |
| Questions And Answer | Back Directory | [Overview]
L-thyroxine is the major hormone derived from the thyroid gland. It is synthesized via the iodination of tyrosines (monoiodotyrosine) and the coupling of iodotyrosines(diiodotyrosine) in the thyroglobulin. Thyroxine is released from thyroglobulin by proteolysis and secreted into the blood. Thyroxine is peripherally deiodinated to form triiodothyronine that exerts a broad spectrum of stimulatory effects on cell metabolism. It is mainly used for the treatment of hypothyroidism, goiter, chronic lymphocytic thyroiditis, myxedema coma, and stupor[1].
The thyroid gland is responsible for the synthesis, storage and release of metabolic hormones including iodine-containing thyroxine(T4) and triiodothyroxine(T3). These hormones are crucial in the regulation of many metabolic processes and are vital for normal growth and development. They are also involved in calorigenic, cardiovascular and metabolic effects. The hormones exert their effects presumably by activating gene transcription of messenger RNA and proteins. To do so, they enter the cell nucleus and bind to DNA-bound thyroid receptors, which regulate gene transcription[2, 3].
| [Biosynthesis]
Normally, the hormones secreted by the thyroid are regulated by the hypothalamic pituitary–thyroid (HPT) axis through a negative feedback system. Low levels of circulating T4 and T3 initiate the release of thyrotropin-releasing hormone (TRH) from the hypothalamus and thyroid-stimulating hormones (TSH) from the pituitary. On interaction with its specific receptor, TSH stimulates the thyroid follicular cells to synthesis T4 and T3 and release them into the bloodstream. When circulating levels of T4 and T3 increase, they inhibit the release of TRH and TSH (i.e. negative feedback mechanism) thereby decreasing their own production[2-5]. The predominant hormone produced by the thyroid gland is T4, with approximately 70–90 mcg of T4 and 15–30 mcg of T3 produced daily[1, 6]. The production of the T3 hormone by the thyroid gland is insufficient to meet the daily requirements of the organs in the body. Therefore, approximately80 % of the body’s required T3 comes from peripheral conversion of T4 to T3[5, 7]. Although both T4 and T3 are active, T3 is more active as thyroid receptors within the cell nucleus have a 10-fold greater affinity for T3.
| [Indication and dosage]
Levothyroxine therapy is used in case of deficiency of the thyroid hormones in the human organism, as it happens under deficiency of thyroid, pituitary and hypothalamic glands (respectively primary, secondary and tertiary hypothyroidism).
Levothyroxine is also used in the treatment of euthyroid goiter and multinodular goiter, including thyroid nodules, subacute or chronic thyroiditis, or in the case of a post-surgical deficit, or after radiometabolic treatment in patients with thyroid cancer[8-10].
For an average adult under the age of 50, the typical levothyroxine sodium dose is approximately 1.7mcg/kg/day, which is equivalent to approximately 100–125 mcg/day. Older patients or patients with cardiac disease may require less levothyroxine and doses should be titrated at intervals of 4–6 weeks. Newborns, infants and adolescents require doses greater than 1.7mcg/kg/day. The guidelines that were recently released by the American Association of Clinical Endocrinologists and American Thyroid Association task force on hypothyroidism in adults, in addition to diagnosis, include suggestions of therapy[11].
| [Formulations]
Commercial levothyroxine oral formulations available in North America and Europe include powders for intravenous solutions, tablets (e.g. Synthroid®, Levo-T™, Levothroid®, Levoxyl®, Unithroid®, Eltroxin®, Elthyrone®, Euthyrox®, Eferox®, Berlthyrox®, Letrox®, Tirosint®), soft gel capsules (Tirosint®) and oral solutions (Eltroxin®, Tirosint® oral drops and Tirosint® oral solution in unit-dose ampules).
There are advantages and disadvantages that are unique to the formulation type and not to levothyroxine per se. For instance, while tablets and capsules offer the advantage of precise dosing, solutions and liquids can be easier to swallow for children or the elderly. Formulation differences that are specific to levothyroxine also exist. The influence of pH on dissolution profiles of tablets and soft gel capsules is dissimilar[12], as well as the negative impact of coffee intake on levothyroxine absorption[13,14].
| [Pharmacokinetics]
Absorption
Levothyroxine is mainly absorbed in the small intestine, more specifically through the duodenum, jejunum and ileum[15,16]. Very little is absorbed in the stomach. Consequently, patients with shorter small intestines (bowel resection) have reduced absorption and require higher levothyroxine doses[17]. The time to maximum concentration (Tmax) occurs at approximately 2 hours in euthyroid volunteers while it is delayed to approximately 3 hours in hypothyroid patients[18]. Food also delays Tmax[18, 19]. The bioavailability of levothyroxine is approximately 60–80 % in euthyroid volunteers[19-21]. It may be slightly higher in hypothyroid and hyperthyroid patients[20, 21], and is decreased in the presence of food from 79 % under fasted conditions to 64 % under fed conditions for a 100-mcg dose[19]. The absorption of levothyroxine appears to be influenced by gastric pH[22, 23]. Centanni et al. demonstrated that in euthyroid patients suffering from nontoxic multinodular goiter, impaired gastric acid secretion or the use of omeprazole was associated with increased dosing requirements in order to adequately suppress TSH[22]. Similarly, Sachmechi and colleagues showed that chronic lansoprazole use in hypothyroid patients also resulted in increased levothyroxine dose requirements to maintain targeted TSH levels[23].
Metabolism and elimination
Although T4 is subject to multiple metabolic reactions[24-26], the main metabolic route for T4 involves deiodination reactions (removal of iodine) by deiodinase enzymes[27-29], Removal of iodine from the carbon 5 of the outer ring transforms T4 to T3, thus T4 can be regarded somewhat as a pro-hormone for T3. Deiodination of the inner ring of T4 can also occur, leading to the formation of inactive reverse T3(rT3). Approximately half of deiodinised T4 is metabolised to rT3 and half to T3[29, 30]. Both T3 and rT3 are further metabolised to diiodothyronine(T2), iodothyronamine(T1) and reverse T2 and T1[29, 30].
The daily turnover rate for T4 is approximately 10 % while it is approximately 50–70 % for T3, with a slightly faster turnover rate in normal volunteers compared with patients with primary hypothyroidism[2, 3]. This equates to a half-life for T4 of 7.5 days in hypothyroid patients and 6.2 days in euthyroid individuals, while the T3 half-life is approximately 1.4 and 1.0 days for hypothyroid and euthyroid volunteers, respectively[34]. Clearance for T4 was similar with 0.056 and 0.054 L/h in hypothyroid and euthyroid subjects, respectively[34] These values are similar to other values reported in hypothyroid patients (0.0385 L/h/70 kg)[31] and in normal control subjects(0.053 to 0.064 L/h)[32, 33].
| [Mechanism of action]
Levothyroxine acts like the endogenous thyroid hormone thyroxine(T4, a tetra-iodinated tyrosine derivative)[1]. In the liver and kidney, T4 is converted to T3, the active metabolite. In order to increase solubility, the thyroid hormones attach to thyroid hormone binding proteins, thyroxin-binding globulin, and thyroxin-binding prealbumin(transthyretin). Transport and binding to thyroid hormone receptors in the cytoplasm and nucleus then takes place. Thus, by acting as a replacement for natural thyroxine, symptoms of thyroxine deficiency are relieved.[1]
| [Adverse reactions]
Adverse reactions[35] may include Abdominal or stomach cramps, change in appetite, crying, diarrhea, false or unusual sense of well-being, fear or nervousness, feeling not well or unhappy, feeling of discomfort, feeling of warmth, feeling things are not real, feelings of suspicion and distrust, hair loss, headache, increased appetite, mental depression, muscle weakness, quick to react or overreact emotionally, rapidly changing moods, redness of the face, neck, arms, and occasionally, upper chest, restlessness, trouble getting pregnant, trouble sitting still, unusual tiredness or weakness, vomiting and weight gain or loss. In rare conditions, symptoms like blurred or double vision, dizziness, eye pain, lack or slowing of normal growth in children, limp or walk favoring one leg, pain in the hip or knee, seizures and severe headache may occur.
| [Precaution]
The following tips should be kept in mind when administrate the levothyroxine[35]:
Levothyroxine should not be used to treat obesity or weight problems. Dangerous side effects or death can occur from the misuse of this medicine, especially if you are taking any other weight-loss medications or appetite suppressants.
Since thyroid hormone occurs naturally in the body, almost anyone can take levothyroxine. However, you may not be able to take this medicine if you have the following conditions, tell your doctor if you have an untreated or uncontrolled adrenal gland disorder, a thyroid disorder called thyrotoxicosis; or, symptoms of a heart attack (chest pain or heavy feeling, pain spreading to the jaw or shoulder, nausea, sweating, general ill feeling). You should also consult your doctor if you have a history of a thyroid nodule, heart disease, a blood clot, or a blood-clotting disorder, diabetes [insulin or oral diabetes medication doses may need to be changed when you start taking this medicine], kidney disease, anemia (lack of red blood cells), osteoporosis, or low bone mineral density, problems with your pituitary gland; or any food or drug allergies. Ask your doctor for advice if you have recently received radiation therapy with iodine (such as I-131). People who become pregnant while taking levothyroxine should not stop taking the medicine without the doctor's advice. Having low thyroid hormone levels during pregnancy could harm both mother and baby. The dose needs may be different during pregnancy.
| [Reference]
- https://www.drugbank.ca/drugs/DB00451
- Haynes R, Thyroid and Antithyroid Drugs. In: Gilman AG, Rall TW, Nies AS, Taylor P [editors]. Goodman and Gilman’s The Pharmacological Basis of Therapeutics, New York: McGraw-Hill, Inc., 1993; 1361–83.
- Dong BJ, Thyroid and Parathyroid Disorders. In: Herfindal ET, Gourley DR, Hart LL [editors]. Clinical Pharmacy and Therapeutics, Baltimore: Williams & Wilkins, 1992; 267–306
- Pangaro LN, Physiology of the Thyroid Gland. In: Becker KL [editor]. Principles and Practice of Endocrinology and Metabolism, Philadelphia: J.B. Lippincott Company, 1990.
- 5. Mandel SJ, Brent GA, Larsen PR, Levothyroxine therapy in patients with thyroid disease, Ann Intern Med, 1993; 119[6]: 492–502.
- Cavalieri RR, Rapoport B, Impaired Peripheral Conversion of Thyroxine to Triiodothyronine, Annu Rev Med, 1977; 28:57–65.
- LoPresti JS, Eigen A, Kaptein E, et al., Alterations in 3,3’5’-triiodothyronine metabolism in response to propylthiouracil, dexamethasone, and thyroxine
- HAYS MT. Thyroid hormone and the gut. Endocrine Res 1988; 14: 203-224.
- LIWANPO L, HERSHMAN JM. Conditions and drugs interfering with thyroxine absorption. Best Pract Res Clin Endocrinol Metab 2009; 23: 781-792.
- JOHN-KALARICKAL J, PEARLMAN G, CARLSON HE. New medications which decrease levothyroxine absorption. Thyroid 2007; 17: 763-765.
- Garber J, Cobin R, Gharib H, et al., Clinical practice guidelines for hypothyroidism in adults: cosponsored by the American Association of Clinical Endocrinologists and the American Thyroid Association, Thyroid, 2012; 22[12]: 1200–35
- Pabla D, Akhlaghi F, Zia H, A comparative pH-dissolution profile study of selected commercial levothyroxine products using inductively coupled plasma mass spectrometry, Eur J Pharm Biopharm, 2009;72[1]:105–10.
- Benvenga S, Bartolone L, Pappalardo M, et al., Altered intestinal absorption of L-thyroxine caused by coffee, Thyroid, 2008;18[3]:293–301.
- Vita R, Saraceno G, Trimarchi F, Benvenga S, A novel formulation of L-thyroxine [L-T4] reduces the problem of L-T4 malabsorption by coffee observed with traditional tablet formulations, Endocrine, 2013;43[1]:154–60.
- Hays MT, Thyroid hormone and the gut, Endocr Res, 1988;14[2–3]:203–24.
- Hays MT, Localization of human thyroxine absorption, Thyroid, 1991;1[3]:241–8.
- Stone E, Leiter LA, Lambert JR, et al., L-thyroxine absorption in patients with short bowel, J Clin Endocrinol Metab, 1984;59[1]:139–41.
- Benvenga S, Bartolone L, Squadrito S, et al., Delayed intestinal absorption of levothyroxine, Thyroid, 1995;5[4]:249–53.
- Wenzel KW, Kirschsieper HE, Aspects of the absorption of oral L-thyroxine in normal man, Metabolism, 1977;26[1]:1–8.
- Read DG, Hays MT, Hershman JM, Absorption of oral thyroxine in hypothyroid and normal man, J Clin Endocrinol Metab, 1970;30[6]:798–9.
- Hasselström K, Siersbaek-Nielsen K, Lumholtz IB, et al., The bioavailability of thyroxine and 3,5,3’-triiodothyronine in normal subjects and in hyperand hypothyroid patients, Acta Endocrinol [Copenh], 1985;110[4]:486–6.
- Centanni M, Gargano L, Canettieri G, et al., Thyroxine in goiter, Helicobacter pylori infection, and chronic gastritis, N Engl J Med, 2006;354[17]:1787–95.
- Sachmechi I, Reich D, Aninyei M, et al., Effect of proton pump inhibitors on serum thyroid-stimulating hormone level in euthyroid patients treated with levothyroxine for hypothyroidism, Endocr Pract, 2007;13[4]:345-9.
- Mol JA, Visser TJ. Rapid and selective inner ring deiodination of thyroxine sulfate by rat liver deiodinase, Endocrinology, 1985;117[1]:8–12.
- Pittman CS, Shimizu T, Burger A, Chambers Jr JB, The nondeiodinative pathways of thyroxine metabolism: 3,5,3’,5-tetraiodothyroacetic acid turnover in normal and fasting human subjects, J Clin Endocrinol Metab, 1980;50[4]:712–16.
- Balsam A, Sexton F, Borges M, Ingbar SH, Formation of diiodotyrosine from thyroxine. Ether-link cleavage, an alternate pathway of thyroxine metabolism, J Clin Invest, 1983;72[4]:1234–45.
- Braverman LE, Ingbar SH, Sterling K, Conversion of thyroxine [T4] to triiodothyronine [T3] in athyreotic human subjects, J Clin Invest, 1970;49[5]:855–64.
- Pittman CS, Chambers JB, Read VH, The extrathyroidal conversion rate of thyroxine to triiodothyronine in normal man, J Clin Invest, 1971;50[6]:1187–96.
- Robbins J, Factors altering thyroid hormone metabolism, Environ Health Perspect, 1981;38:65–70.
- Engler D, Merkelbach U, Steiger G, Burger AG, The monodeiodination of triiodothyronine and reverse triiodothyronine in man: a quantitative evaluation of the pathway by the use of turnover rate techniques, J Clin Endocrinol Metab, 1984;58[1]:49–61.
- Fish LH, Schwartz HL, Cavanaugh J, et al., Replacement dose, metabolism, and bioavailability of levothyroxine in the treatment of hypothyroidism. Role of triiodothyronine in pituitary feedback in humans, N Engl J Med, 1987;316[13]:764–70.
- Chambers Jr J, Pittman C, Suda A, The effects of propranolol on thyroxine metabolism and triiodothyronines production in man, J Clin Pharmacol, 1982;22[2–3]:110–16.
- van der Heijden J, Krenning E, van Toor H, et al., Three-compartmental analysis of effects of D-propranolol on thyroid hormone
- Nicoloff JT, Low JC, Dussault JH, Fisher DA, Simultaneous Measurement of Thyroxine and Triiodothyronine Peripheral Turnover Kinetics in Man, J Clin Invest, 1972;51[3]:473–83
- https://www.drugs.com/sfx/levothyroxine-side-effects.html
|
| Hazard Information | Back Directory | [Description]
L-Thyroxine is a synthetic form of the thyroid hormone thyroxine.1,2,3 In vivo, L-thyroxine (0.9 and 2.7 μg) inhibits synthesis and release of thyrotropin induced by thyrotropin-releasing hormone (Item No. 22917) from the anterior pituitary in mice.1 It also reverses decreases in levels of circulating thymic serum factor (FTS) and the number of T rosette-forming cells in an old age-induced mouse model of hypothyroidism.2,3 Formulations containing L-thyroxine have been used in the treatment of hypothyroidism. | [Chemical Properties]
Crystalline Solid | [Originator]
Synthroid,Flint,US,1953 | [Uses]
antihypercholesterimic, thyromimetic | [Uses]
One of the thyroid hormones involved in the maintenance of metabolic homeostasis. Synthesized and stored as amino acid residues of thyroglobulin, the major protein component of the thyroid follicular
colloid. Synthesis and secretion are regulated by the pituitary hormone (TSH). Deiodinated in peripheral tissues to the active metabolite, liothyronine. The D-form has very little activity as a thyroi
d hormone, but has been used to treat hyperlipidemia. | [Definition]
ChEBI: The L-enantiomer of thyroxine. | [Indications]
Effects of this drug depend heavily on dosage. In small doses, levothyroxine exhibits anabolic
action. In medium doses, it stimulates growth and development of tissue, metabolism
of protein, fats, and carbohydrates, increases functional activity of central nervous and cardiovascular
systems, as well as kidneys and liver. In large doses, it slows the thyrotropic
activity of the hypophysis and suppresses thyroid gland production. Levothyroxine is used
for hypothyroidism, myxedema, thyrotoxicosis, erythyroid conditions, and cretinism. | [Manufacturing Process]
A 9.30 g portion of N-acetyl-L-diiodotyrosinamide was suspended in 100 ml of
0.05M boric acid (H3BO3) and 100 ml of 95% ethanol, and the solid was
dissolved by adjusting the pH to 10.5 with 2N sodium hydroxide (NaOH). A
15% (by weight) portion of manganese sulfate monohydrate was added and
the solution heated at 44°C under conditions of oxygenation while being
agitated mechanically. After approximately 24 hours of incubation, the
precipitated product was collected and separated from the catalyst, providing
the amide of N-acetyl-L-thyroxine in 30.6% yield. On hydrolysis (removal of
both amide functions), achieved by refluxing in glacial acetic acid-hydrochloric
acid (approximately 2:1), L-thyroxine is obtained. It was isolated as the
sodium salt, containing approximately 5 molecules of water of hydration. | [Brand name]
Levo-T (Alara);
Levolet (Vintage); Levothroid (Lloyd); Levoxyl (Jones);
Novothyrox (Genpharm); Synthroid (Abbott); Unithroid
(Stevens J). | [Therapeutic Function]
Thyroid hormone | [Synthesis]
Levothyroxine, L-3-[4-(4-hydroxy-3,5-diiodophenoxy)-3,5-diiodophenyl]
alanine (25.1.10), is synthesized in a multi-stage synthesis from 4-hydroxy-3-iodo-
5-nitrobenzaldehyde. Reacting this with benzenesulfochloride in pyridine gives the corresponding
benzenesulfonate 25.1.1, the benzenesulfonyl group of which is easily replaced
with a 4-methoxyphenyloxy- group upon reaction with 4-methoxyphenol. The resulting
3-iodo-4-(4-methoxyphenoxy)benzaldehyde (25.1.2) is reacted further with N-acetylglycine
in the presence of sodium acetate in a Knoevenagel reaction, in which the resulting ylidene
compound cyclizes to an oxazolone derivative 25.1.3. The oxazolone ring of this compound
is opened upon reaction with sodium methoxide, forming the desired cinnamic acid derivative
25.1.4. The nitro group of this product is reduced to an amino group by hydrogen in the
presence of a Raney nickel catalyst, forming the corresponding amine, and subsequent diazotation
and replacement of the diazo group of which with iodine gives the methyl ester of
|á-acetamido-3,5-diiodo-4-(4-methoxyphenoxy)crotonic acid (25.1.6). The resulting compound
undergoes simultaneous reaction with hydrogen iodide and phosphorous in acetic
acid, in which the double bond in the crotonic acid is reduced, and the methoxy protection is
removed from the phenol ring. During this, a simultaneous hydrolysis of the acetyl group on
the nitrogen atom also takes place, forming D,L-3,5-diiodothyronine (25.1.7). The amino
group in this product is once again protected by the reaction with formic acid in the presence
of acetic anhydride, which gives D,L-N-formyl-3,5-diiodothyronine. Separation of isomers in
the resulting racemic mixture is accomplished using brucine, giving D-(+)-N-formyl-3,
5-diiodothyronine L-(+)-N-formyl-3,5-diiodothyronine (25.1.8). The protecting formyl
group is hydrolyzed using hydrobromic acid, giving L-(+)-3,5-diiodothyronine (25.1.9),
which undergoes direct iodination using iodine in the presence of potassium iodide in
aqueous methylamine, to give the desired levothyroxine.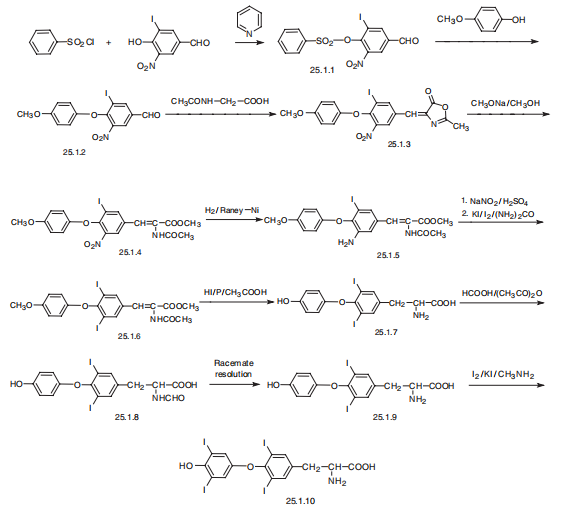
| [Purification Methods]
Purification is the same as for the D-isomer above. Likely impurities are tyrosine, iodotyrosine, iodothyroxines and iodide. Dissolve it in dilute ammonia at room temperature, then crystallise it by adding di[�] 546 +27.8o (c 5, EtOH). [Harrington et al. Biochem J 39 164 1945, Nahm & Siedel Chem Ber 96 1 1963, Reineke & Turner J Biol Chem 161 613 1945, Chalmers et al. J Chem Soc 3424 1949, Beilstein 14 II 378, 14 III 1566, 14 IV 2373.] |
|
|