| Identification | Back Directory | [Name]
MEFLOQUINE | [CAS]
53230-10-7 | [Synonyms]
Mefloquin
Mephaquin
Ro 21-5998
Metloquine
MEFLOQUINE
RaceMic Mefloquine
(11S,2'R)-Mefloquine
(11R,2'S)-Mefloquine
MEFLOQUINE USP/EP/BP
(±)-erythro-Mefloquine
MEFLOQUINE INTERMEDIATE
Mefloquine Labeled d7 (mixture of isotope locations)
(S)-α-[(2R)-2-Piperidyl]-2,8-bis(trifluoromethyl)-4-quinolinemethanol
(R)-α-[(2S)-2-Piperidyl]-2,8-bis(trifluoromethyl)-4-quinolinemethanol
(R)-(2,8-bis(trifluoromethyl)quinolin-4-yl)((S)-piperidin-2-yl)methanol
rel-[2,8-bis(trifluoromethyl)quinolin-4-yl]-[(2R)-piperidin-2-yl]methanol
(R*,S*)-(alpha-(2-Piperidinyl)-2,8-bis(trifluoromethyl)-4-quinolinemethanol
4-Quinolinemethanol, α-(2R)-2-piperidinyl-2,8-bis(trifluoromethyl)-, (αS)-rel-
4-QuinolineMethanol, a-(2R)-2-piperidinyl-2,8-bis(trifluoroMethyl)-, (aS)-rel-
MefloquineQ: What is
Mefloquine Q: What is the CAS Number of
Mefloquine Q: What is the storage condition of
Mefloquine
ROS,ERK,AMPK,KcsA,Mefloquin,Potassium Channel,ROS Kinase,SARS-CoV,SARS coronavirus,Calu-3,anticancer,VeroE6/TMPRSS2,JNK,Parasite,Mefloquine,antimalarial,PCa cell,prostate cancer,inhibit,Inhibitor,Autophagy | [Molecular Formula]
C17H16F6N2O | [MDL Number]
MFCD00869324 | [MOL File]
53230-10-7.mol | [Molecular Weight]
378.31 |
| Chemical Properties | Back Directory | [Melting point ]
242-244°C | [Boiling point ]
415.7±40.0 °C(Predicted) | [density ]
1.383±0.06 g/cm3(Predicted) | [storage temp. ]
Refrigerator, Under Inert Atmosphere | [pka]
pKa 8.6 (Uncertain) | [CAS DataBase Reference]
53230-10-7 |
| Hazard Information | Back Directory | [Chemical Properties]
Off-White Solid | [Uses]
Labelled quinoline methanol antimalarial agent. | [Brand name]
Lariam (Roche). | [Description]
Mefloquine, which was synthesized with the intent of blocking the site of metabolism in quinine
with the chemically stable CF3 group, exists as four optical isomers of nearly equal activity. The
drug is active against chloroquine-resistant strains of plasmodium, yet cross-resistance is not
uncommon. Metabolism is cited as the possible mechanism of resistance. Mefloquine is slowly
metabolized through CYP3A4 oxidation to its major inactive metabolite, carboxymefloquine. Most of the parent drug is excreted unchanged into the urine. Its coadministration with
CYP3A4 inhibitors (e.g., ketoconazole) has increased the area under the curve for mefloquine by
inhibiting its metabolism to carboxymefloquine. | [Originator]
Lariam,Roche Pharmaceuticals,Switz. | [Definition]
ChEBI:(-)-(11S,2'R)-erythro-mefloquine is an optically active form of [2,8-bis(trifluoromethyl)quinolin-4-yl]-(2-piperidyl)methanol having (-)-(11S,2'R)-erythro-configuration. An antimalarial agent, used in racemic form, which acts as a blood schizonticide; its mechanism of action is unknown. It has a role as an antimalarial. It is an enantiomer of a (+)-(11R,2'S)-erythro-mefloquine. | [Manufacturing Process]
The first method of synthesis of 2,8-bis(trifluoromethyl)-4-quinolinyl-2- pyridinylmethanone
N-Methoxy-N-methyl-2,8-bis(trifluoromethyl)-quinoline-4-carboxamide was
prepared using synthetic methodology reported by Thiesen et al (J. Org.
Chem. 1988, 53, 2374). To a suspension of 12.5 g (40.4 mmol) 2,8-
bis(trifluoromethyl)quinoline-4-carboxylic acid (was prepared by the method of
Hickmann et al. (U.S. Patent No. 4,327,215)) in 200 ml CH2Cl2 was added
1,1'-carbonyldiimidazole (7.3 g, 45 mmol) and N,O-dimethylhydroxylamine
hydrochloride (4.25 g, 45 mmol). The resulting deep red solution was stirred
overnight, then poured into dilute hydrochloric acid (0.25 M, 200 ml). The
organic phase was separated, and washed with dilute sodium hydroxide and
brine, and dried (MgSO4). The solvents was evaporated to leave a viscous
brown oil, which was filtered through a pad of silica gel using ethyl acetatehexane (1:1) as eluent to give N-methoxy-N-methyl-2,8-bis(trifluoromethyl)-
quinoline-4-carboxamide as a yellowish oil, 14.3 g (98%), which solidified on
standing. This material was broken up under hexane to afford the product as
a solid, melting point 93-95°C. Analysis of this material by HPLC showed it to
be >99.8% pure.
To a solution of the N-methoxy-N-methyl-2,8-bis(trifluoromethyl)-quinoline-4-
carboxamide amide (10 g, 28.4 mmol) in anhydrous ether (100 ml) was
added a solution of 2-pyridyl lithium (Pinder et al (J. Med. Chem. 1968, 11,
267)) [formed by addition of 2-bromopyridine (3.3 ml, 34.6 mmol) to a
solution of butyl lithium (29.7 ml of a commercial 1.6 M solution, diluted with
an equal quantity of ether) at -78°C] at -78°C. Analysis of the reaction by TLC
after 10 min showed that no starting material remained. The reaction was
allowed to warm to room temperature, then poured into aqueous ammonium
acetate, and extracted with ether, the combined organic layers washed with
brine and dried (MgSO4). Filtration through a pad of silica gel using ethyl
acetate-hexane (1:1) afforded 9.0 g (84%) of the crude 2,8-
bis(trifluoromethyl)-4-quinolinyl-2-pyridinylmethanone. This was recrystallised
from isopropyl alcohol to give the product as colourless needles, identical to
that described in the literature (Hickmann et al.; Pinder et al.; Ohnmacht et
al.; and Adam et al. (Tetrahedron 1991, 36, 7609)).
The second method of synthesis of 2,8-bis(trifluoromethyl)-4-quinolinyl-2-
pyridinylmethanone
In a round bottom flask (100 ml) were placed 4-chloro-2,8-
bis(trifluoromethyl)quinoline (0.0385 mole, 11.52 g), 2-pyridylacetonitrile
(0.0423 mole, 5.0 g), benzyltriethylammonium chloride (0.26 g, 3 mole %),
THF (35 ml) and aq NaOH (20 N, 9.63 ml, 0.192 moles). On stirring the
colour of the solution became cherry red. The reaction temperature was
increased to 5-0°C and stirred for further 1 hour. Monitoring of the reaction
mixture by thin layer chromatography (TLC) or gas liquid chromatography
(GLC) indicated complete consumption of 4-chloroquinoline to give nitrile. The
reaction temperature was lowered to 20-25°C followed by addition of 30%
H2O2 (13 ml, 0.1154 moles). TLC and GLC monitoring indicated complete
conversion of nitrile compound to 2,8-bis(trifluoromethyl)-4-quinolinyl-2-
pyridinylmethanone. Reaction mixture was cooled to 0-5°C and neutralized by
ortho-phosphoric acid (85% aq, 4.5 ml). THF was distilled off, followed by
addition of water (30 ml) and extraction with toluene. The crude product was
crystallized from isopropanol to obtain 2,8-bis(trifluoromethyl)-4-quinolinyl]-2-
pyridinylmethanone. Yield = 13.17 g (92%), melting point 123°C. | [Therapeutic Function]
Antimalarial | [World Health Organization (WHO)]
Mefloquine was developed in response to proliferation of multidrug
resistant strains of Plasmodium falciparum, and has been widely used since
the early 1980s. Provided the drug is used appropriately, the risks associated with
its prophylactic use are clearly outweighed by the benefits. Mefloquine is listed in
the WHO Model List of Essential Drugs. | [Antimicrobial activity]
Mefloquine is a lipophilic drug with a high affinity to membranes.
A concentration of 10–40 nm has rapid dose-related
activity against erythrocytic stages of Plasmodium spp.,
including strains resistant to chloroquine, sulfonamides and
pyrimethamine. The C-11 (hydroxy) enantiomers have equal
antimalarial activity. It also exhibits activity against bacteria
(including methicillin-resistant Staphylococcus aureus), and
some fungi and helminths. | [Acquired resistance]
Resistance in P. falciparum is widespread in South East Asia
where high-grade resistance was found in 15% of patients and
low-grade resistance in about 50%. There is cross-resistance
with quinine and halofantrine, and an inverse relationship
with chloroquine resistance has been reported. The molecular
basis of resistance remains unclear but polymorphisms
of the pfmdr1 gene, associated with chloroquine resistance,
led to increased sensitivity to mefloquine. Resistant strains of
P. falciparum appeared in Africa before the drug was used in
that continent, perhaps because of quinine abuse or intrinsic
resistance. In South East Asia, declining response rates to
combination therapy with mefloquine and artesunate are
reported. | [Pharmaceutical Applications]
A synthetic 4-quinolinemethanol, formulated as the hydrochloride
for oral administration. It is slightly soluble in water. | [Pharmacokinetics]
Oral absorption: 70–80%
Cmax 1 g oral: 1 mg/L after 2–12 h
Plasma half-life: 20 days
Volume of distribution: 16–25 L/kg
Plasma protein binding: 98%
Mefloquine is concentrated two- to five-fold in erythrocytes.
The major metabolites do not have antimalarial activity.
Pregnant women require larger doses than non-pregnant
women to achieve comparable blood levels. It is predominantly
excreted in the bile. Less than 10% is excreted in urine. | [Clinical Use]
Antimalarial prophylaxis in areas of chloroquine resistance
Treatment of uncomplicated multidrug-resistant malaria
A mefloquine–artesunate co-formulation is available.
Mefloquine has been used for the treatment of cutaneous
leishmaniasis in South America. | [Synthesis]
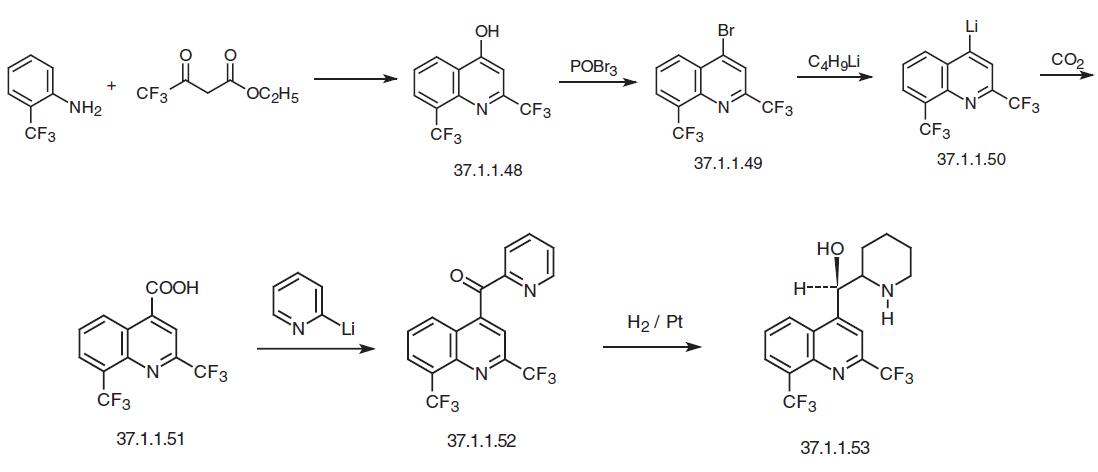
Mefloquine, D,L-erythro-α-2-piperidyl-2,8-bis-(trifluoromethyl)-4-quinolin�methanol (37.1.1.53), is made in various ways from 2-trifluoromethylaniline. According to the first method, heterocyclization of the reaction product 2-trifluoromethylaniline with trifluo�roacetoacetic ester gives 2,8-bis-(trifluoromethyl)-4-hydroxyquinoline (37.1.1.48). Reacting the product with phosphorus tribromide replaces the hydroxyl group in the fourth position of the quinoline ring with a bromine atom, giving 2,8-bis-(trifluoromethyl)-4-bromoquinoline (37.1.1.49). Reaction of the last with butyllithium gives a organolithium derivative—2,8- bis-(trifluoromethyl)-4-lithiumquinoline (37.1.1.50). Reacting this with carbon dioxide makes 2,8-bis-(trifluoromethyl)-4-quinolincarboxylic acid (37.1.1.51). Interaction of the resulting acid with 2-lithiumpyridine gives the ketone (37.1.1.52). Reducing both the keto group and the pyridine ring with hydrogen using a platinum catalyst gives the desired mefloquine.
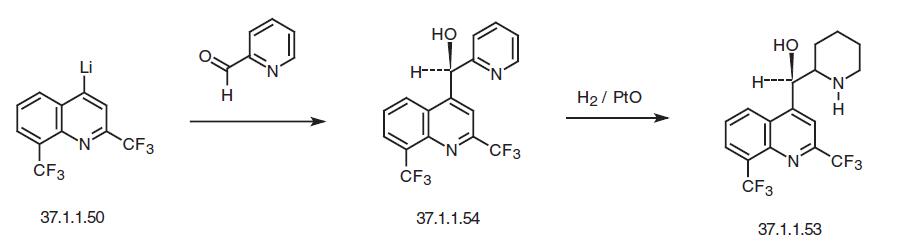
The second way of making mefloquine is from 2,8-bis-(trifluoromethyl)-4-lithiumquini�line described above (37.1.1.50), which is reacted with 2-formylpyridine to make α-2-pyridyl-2,8-bis-(trifluoromethyl)-4-methanolquinoline (37.1.1.54). The pyridiyl group in this compound is also reduced as described above, resulting in the formation of the desired mefloquine.
Finally, the third way of making mefloquine also begins with 2-trifluoromethylaniline, except in this case it is reacted with chloralhydrate and hydroxylamine to make isoni�trosoacetyl(2-trifluoromethyl)anilide (37.1.1.55), which when heated in the presence of sulfuric acid cyclizes to 7-trifluoromethylisatine (37.1.1.56) (Sandmeyer reaction). The resulting 7-trifluoromethylisatine (37.1.1.56) is then reacted with 1,1,1-trifluoroacetone in the presence of a base in a Friedlaender reaction conditions to make 2,8-bis-(trifluoromethyl)-4-quinoline carboxylic acid described above (37.1.1.51). Reacting this with lithium hydroxide turns it into a lithium salt, which is reacted with a Grignard reagent, 2-magnesiumbromopyridine (made from 2-bromopyridine and magnesium). The resulting ketone (37.1.1.52) is again reduced with a platinum catalyst to make the desired mefloquine.
|
| Questions And Answer | Back Directory | [Pharmacology and mechanism of action]
Mefloquine is a quinolinemethanol derivative which is structurally related to quinine. It was synthesized and tested by the United States army in the 1960s. The available mefloquine preparation is a racemate with two enantiomers in equal proportions [1]. It was introduced for the treatment of multiresistant P. falciparum in the mid-1980s [2]. In Africa, there are only occasional reports of therapeutic failures, but there has been a rapid development of resistance in the 1990s in parts of Southeast Asia, particularly in Thailand [3]. Cross-resistance with quinine and halofantrine has also been reported [4, 5]. The mechanism of action is not well established. Mefloquine is a schizontocidal drug active against the erythrocytic stages of all species of malaria parasites. It is inactive against exoerythrocytic forms and thus cannot prevent relapse of P. vivax and P. ovale infections [6].
| [Indications]
Treatment and prophylaxis against chloroquine resistant P. falciparum malaria.
| [Contraindications]
There is little experience in children under 2 years, and mefloquine is therefore not recommended in this group unless other alternatives are ineffective . Mefloquine should not be used by persons involved in activities requiring fine co-ordination and spatial performance such as air crews or by persons with a history of epilepsy or psychiatric disorders . People taking cardioactive drugs like digoxin, quinidine, beta-blockers, or calcium channel blockers should avoid mefloquine . Those on mefloquine prophylaxis or given mefloquine treatment should only be given quinine under close medical supervision because of the risk of additive neurological and cardiological toxicity [3].
| [Side effects]
The severity and frequency of side effects during treatment are dose-related. In early clinical trials (a total of 436 patients), the most frequent adverse reactions were nausea (18%), diarrhoea (15%), dizziness (15%), vomiting (13%), sinus bradycardia (9%), abdominal pain (8%), skin itching or rash (1%) and behaviour disorders with paranoid ideas and hallucinations (1%) [7]. Early vomiting within 1 hour after drug administration reduced the mefloquine concentrations in patients with P. falciparum malaria. This indicates that vomiting within 1 hour requires a repeated dose [8]. The most important side effects of mefloquine are neuropsychiatric reactions. In 7 volunteers given 15 mg mefloquine/kg, all experienced some neurological symptoms (concentration difficulties, dizziness, vertigo) within 6 hours after administration of the drug [9]. Serious neuropsychiatric adverse reactions, in particular general convulsions, confusion, and hallucinations, have been reported after therapeutic use of mefloquine [10,11]. The incidence may be as high as 1% and the onset usually occurs within 4 days of intake [12]. Neurological and psychiatric reactions seem to be dose-dependent . All neuropsychiatric reactions are reversible once the drug administration is discontinued. No fatalities have been reported [13]. Less frequent adverse effects mainly associated with curative doses are anorexia, asthenia, irregular heart rate, pulse irregularities, constipation, insomnia, diarrhoea, arthralgia, and hearing disturbances [14]. Single case reports of Stevens-Johnson syndrome, severe facial rash, and agranulocytosis have been filed [15]. During prophylaxis, the frequency of reported symptoms among 2780 travellers using mefloquine was similar to that of chloroquine and only one possible serious reaction (depression) was reported [16]. In 1991, the recommended prophylactic dose of mefloquine for adults was increased to 250 mg once weekly during the whole period. The experience with this dose is still limited, but it was well tolerated in a trial in US peace corps volunteers in West Africa [17]. There are no large, double-blind, prospective, randomized studies that compare the risk for adverse reactions between different antimalarial drugs used for prophylaxis. Large retrospective studies in US Peace Corps volunteers and European travellers found no major difference in the incidence of side effects in mefloquine compared to chloroquine users . Until May 1991, a total of 59 serious neuropsychiatric adverse reactions (26 convulsions, 12 depressions, 20 psychotic episodes, and one toxic encephalopathy) have been reported to Roche after prophylaxis The majority (80%) of all neuropsychiatric reactions appeared within 3 weeks of onset of prophylaxis[18]. In Germany, the risk of moderate to severe neuropsychiatric reactions during prophylaxis was calculated to be one in 13,000 users [19].
| [Preparations]
Available as mefloquine hydrochloride: 274 mg hydrochloride is equal to 250 mg base. • Lariam® (Roche) (or Laricum in some countries). Tablets 250 mg base (228 mg base in the US). • Mephaquin® (Mepha). Tablets 250 mg base.
| [References]
1. Sweeney T (1981). The present status of malaria chemotherapy: mefloquine, a novel antimalarial. Med Res Rev, 1, 281–301.
2. Practical Chemotherapy of Malaria. Technical report series No. 805 (1990). (Geneva: World Health Organization).
3. International Travel and Health (1994). (Geneva: World Health Organization).
4. Rojas-Rivero L, Gay F, Bustos MDG, Ciceron L, Pichet C, Danis M, Gentilini M (1992). Mefloquine-halofantrine cross-resistance in Plasmodium falciparum induced by intermittant mefloquine pressure. Am J Trop Med Hyg, 47, 372–377.
5. Brasseur P, Kouamouo J, Druilhe P (1991). Mefloquine-resistant malaria induced by inappropriate quinine regimens. J Infect Dis, 164, 625–626.
6. Black RH, Canfield CJ, Clyde DF, Peters W, Wernsdorfer WH (1986). Mefloquine. In: Chemotherapy of Malaria, 2nd edn, edited by L.Bruce-Chwatt. (Geneva: World Health Organization 1986).
7. Advances in Malaria Chemotherapy. Technical Report Series No. 711 (1984). (Geneva: World Health Organization).
8. Karbwang J, Na Bangchang K, Bunnag D, Harinasuta T (1991). Pharmacokinetics and pharmacodynamics of mefloquine in Thai patients with acute falciparum malaria. Bull World Health Organ, 69, 207–212.
9. Patchen LC, Campell CC, Williams SB (1989). Neurological reactions after a therapeutic dose of mefloquine. N Engl J Med, 321, 1415.
10. Rouveix B, Bricaire F, Michon C, Franssen G, Le Bras J, Bernard J, Ajana F, Vienne JL (1989). Mefloquine and an acute brain syndrome. Ann Intern Med, 110, 577–578.
11. Stuvier PC, Ligthelm RJ, Goud Th JLM (1989). Acute psychosis after mefloquine. Lancet, ii, 282.
12. World Health Organization. Review of central nervous system adverse events related to antimalarial drug, mefloquine (1985–1990) (WHO/MAL911063). (Geneva: World Health Organization).
13. Bem JL, Kerr L, Stürchler D (1992). Mefloquine prophylaxis: an overview of spontaneous reports of severe psychiatric reactions and convulsions. J Trop Med Hyg, 95, 167–179.
14. Mefloquine. Therapeutic Drugs, edited by Sir Colin Dollery (1991) (London: Churchill Livingstone), pp. M35–M39.
15. Martindale: The Extra Pharmacopoeia, 30th edn, (1993) (London: Pharmaceutical Press), pp. 402–403.
16. Steffen R, Heusser R, M?chler R, Bruppacher R, Naef U, Chen D, Hofmann AM, Somaini B (1990). Malaria chemoprophylaxis among European tourists in tropical Africa: use, adverse reactions and efficacy. Bull World Health Organ, 68, 313–322.
17. Lobel HO, Miani M, Eng T, Bernard KW, Hightower AW, Campbell CC (1993). Long-term prophylaxis with weekly mefloquine. Lancet, 341, 848–851.
18. Stürchler D, Handschin J, Kaiser D, Kerr L, Mittelholzer M-L, Reber R, Fernex M (1990). Neuropsychiatrie side effects of mefloquine. N Engl J Med, 322, 1752–1753.
19. Weinke T, Trautmann M, Held T, Weber G, Eichenlaub D, Fleischer K, Kern W, Pohle HD (1991). Neuropsychiatrie side effects after the use of mefloquine. Am J Trop Med Hyg, 45, 86–91.
|
|
| Company Name: |
ANWITA APIS
|
| Tel: |
+919000311012 |
| Website: |
www.anwita-api.com |
|